Ebola
| 卫生署举行伊波拉应变演习
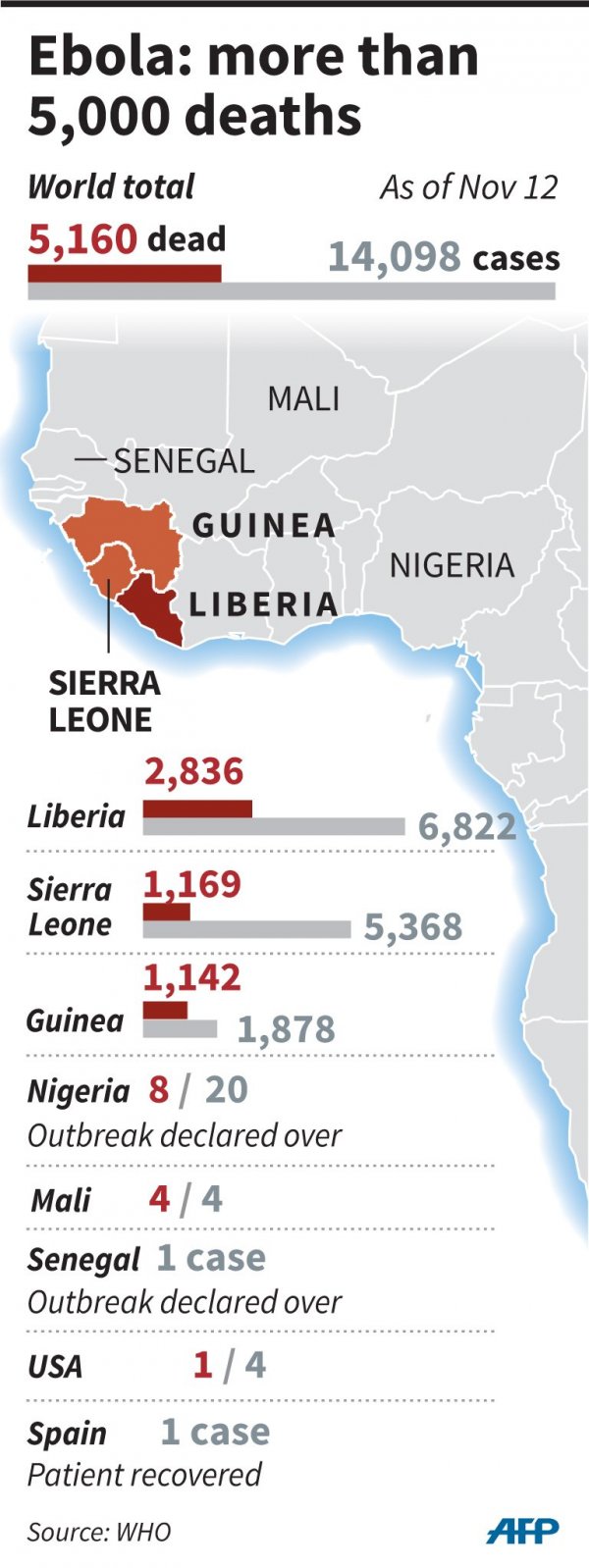
Ebola deaths Figures published 8 January 2015 8,274 Deaths The World Health Organization (WHO) admits the figures are underestimates, given the difficulty collecting the data. WHO officials this week discovered scores of bodies. Source: WHO
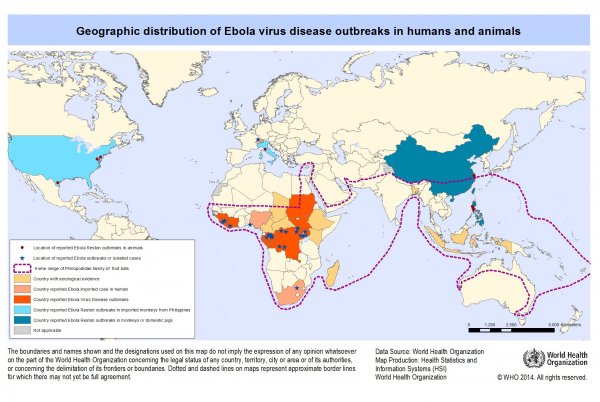
Mission Unaccomplished: Containing Ebola in Africa January 01, 2015 World Health Organization Ebola's global reach After Ebola, World Bank Chief Proposes Global Insurance Program For Future Outbreaks World Bank Group President Jim Yong Kim is proposing emerging nations, developed countries and global aid organizations participate in a kind of insurance system to help pay for health crises like West Africa's Ebola outbreak. “We need to prepare for future pandemics that could become far more deadly and infectious than we we have seen so far with Ebola,” Kim told an audience at Georgetown University on Tuesday. “We must learn the lessons from the Ebola outbreak because there is no doubt we will be faced with other pandemics in the years to come.” The largest Ebola outbreak ever recorded has killed more than 8,700 people in West Africa, and will cost Guinea, Liberia and Sierra Leone billions in the short term. Experts say weak health infrastructure in these countries contributed to the large scale of the outbreak. Governments and charities from around the world have donated billions in aid, and the number of cases has recently started to decrease. But according to Kim, the recent outbreak could be just the beginning. And world leaders need a plan. He explained World Bank officials informally discussed the possibility of a “pandemic response facility” with the World Health Organization, United Nations and other international actors last week at the World Economic Forum in Davos, Switzerland. “This could work like insurance policies that people understand, like fire insurance,” Kim said. “The more that you are prepared for a fire, such as having several smoke detectors in your home, the lower the premium you pay.” He said countries, companies and organizations could work together to prepare for future problems by developing stronger health system infrastructure, surveillance and fast-acting medical response teams. This would lower the “premium” they pay. “That would benefit donors and others who would pay the premium, but the greatest benefit would be that market mechanisms would help us push improvements in our preparedness for epidemics,” he said. While nothing is official yet, Kim said the World Bank may send proposals to world leaders in the next few months. Modelling the spread of Ebola using air-transport networks THE Ebola virus is not contagious through the air, but air travel has played its part in spreading it within west Africa and beyond. Dirk Brockmann, a specialist in complex networks at Humboldt University in Berlin, has used air-transport data to quantify the probabilities of an infected passenger who has boarded a plane in one of the three most affected countries—Guinea, Liberia and Sierra Leone—exiting the network at a specific airport around the world. For every 100 infected passengers embarking in Guinea, Liberia and Sierra Leone, 84 would normally disembark at another African airport. Three would arrive in Britain and France; only one in America. Thursday 8 January 2015 09.12 GMT Scientists have discovered a new class of antibiotic using a revolutionary procedure hailed as a game changer in the hunt for medicines to fight drug-resistant infections. The antibiotic, called teixobactin, kills a wide range of drug-resistant bacteria, including MRSA and bugs that cause TB and a host of other life-threatening infections. It could become a powerful weapon in the battle against antimicrobial resistance, because it kills microbes by blocking their capacity to build their cell walls, making it extremely difficult for bacteria to evolve resistance. “Teixobactin kills exceptionally well. It has the ability to rapidly clear infections,” said research leader Kim Lewis, director of the Antimicrobial Discovery Center at Northeastern University in Boston, US. The public health threat of resistance was highlighted last year in a World Health Organisation report that warned the world was entering a “post-antibiotic era”. The UK’s chief medical officer, Sally Davies, has put antibiotic resistance on the government’s national risk register, alongside terrorist attacks and pandemic flu, and warned that without new antibiotics, more people will die after routine operations in the next 20 years. In December, a report commissioned by David Cameron warned that failure to tackle drug-resistant infections will cost the global economy up to £64tn ($100tn) by 2050. In studies on mice, the new antibiotic wiped out infections of Staphylococcus aureus and Streptococcus pneumoniae, which can cause life-threatening blood and lung infections. It was also effective against Enterococcus, which can infect the heart, prostate, urinary tract and abdomen. Most antibiotics are isolated from bacteria or fungi that churn out lethal compounds to keep other microbes at bay. But scientists have checked only a tiny fraction of bugs for their ability to produce potential antibiotics because 99% cannot be grown in laboratories. Lewis’s group found a way around the problem by developing a device called an iChip that cultures bacteria in their natural habitat. The device sandwiches the bugs between two permeable sheets. It is then pushed back into the ground where the microbes grow into colonies. The researchers found that after two weeks in the ground, the microbial colonies had grown enough to run tests on them. To do this, they covered the top of the iChip with layers of pathogens. Bugs that produced natural antibiotics revealed themselves by killing the pathogens above them. Working with a Massachusetts-based company, NovoBiotic, and researchers at the University of Bonn, Lewis’s group screened 10,000 soil bacteria for antibiotics and discovered 25 new compounds. Of these, teixobactin was the most promising. Teixobactin’s ability to kill bugs is only part of the attraction of the compound. Writing in the journal Nature, the scientists describe how none of the bacteria treated with the antibiotic showed signs of developing resistance. The reason for the drug’s apparent resilience was discovered by Tanja Schneider in Bonn. Most antibiotics target bacterial proteins, but bugs can become resistant by evolving new kinds of proteins. Teixobactin works differently. It launches a double attack on the building blocks of bacterial cell walls themselves. “That’s an Achilles’ heel for antibiotic attack,” Schneider said. “It would take so much energy for the cell to modify this, I think it’s unlikely resistance will appear this way.” Though promising, Lewis said that years more work lie ahead before the drug could be available. Human clinical trials could begin within two years to check its safety and efficacy, but more development would follow that. At the moment the drug would have to be given as an injection, but an oral pill would be more attractive. Another shortcoming of teixobactin is that it only works against bacteria that lack outer cell walls, known as Gram-positive bacteria, such as MRSA, Streptococcus and TB. It doesn’t work against Gram-negative bacteria, which include some of the most worrying antibiotic-resistant pathogens, such as Klebsiella, E. coli and Pseudomonas. Despite these limitations, the discovery of the antibiotic, and the process used to grow previously ungrowable microbes, has raised hopes among researchers in the field. “What most excites me is the tantalising prospect that this discovery is just the tip of the iceberg,” said Mark Woolhouse, professor of infectious disease epidemiology at the University of Edinburgh. “It may be that we will find more, perhaps many more, antibiotics using these latest techniques.” The model does not show the current, absolute risks of Ebola arriving in a country. It starts with the assumption that infected people are on the plane in the first place: the actual risks are therefore far lower. It also reflects a normal travel schedule, when in fact many countries and airlines have suspended or modified flights. But Mr Brockmann's work does underline two things. First, the risks of Ebola spreading are overwhelmingly focused in Africa itself. Second, if a Western country is truly intent on keeping Ebola out, it has to go further than banning direct flights from the worst-affected places and must also target global hubs. Airports in London and Paris play a big part in linking Sierra Leone and Guinea to the rest of the world. America’s single Ebola fatality may have disembarked in Dallas but the first leg of his journey from Monrovia, Liberia’s capital, was to Brussels. Photo: AP Health workers load a suspected Ebola patient into the back of an ambulance in Freetown, Sierra Leone. Professors from three leading British universities say policies favoring international debt repayment over social spending contributed to the Ebola crisis by hampering health care in the three worst-hit West African countries. Conditions for loans from the International Monetary Fund prevented an effective response to the outbreak that has killed nearly 8,000 people, the academics allege in a report in The Lancet Global Health journal this month. Show more Photo: APHealth workers load a suspected Ebola patient into the back of an ambulance in Freetown, Sierra Leone. Professors from three leading British universities say policies favoring international debt repayment over social spending contributed to the Ebola crisis by hampering health care in the three worst-hit West African countries. Conditions for loans from the International Monetary Fund prevented an effective response to the outbreak that has killed nearly 8,000 people, the academics allege in a report in The Lancet Global Health journal this month. Show more BERLIN (AP) — The World Health Organization says the number of reported Ebola deaths in West Africa has risen to 7,905. The WHO says altogether some 20,206 cases of Ebola virus disease have been reported since the outbreak in December 2013. Guinea, Liberia and Sierra Leone have been the hardest-hit countries in the epidemic. An update released late Wednesday by the WHO says that new cases in Liberia have mostly declined in the past six weeks. In Sierra Leone, there are signs the increase of new cases has slowed, but the agency says "the country's west is now experiencing the most intense transmission of all the affected countries." The situation of the epidemic in Guinea is fluctuating, with between 70 and 160 confirmed cases over the past 15 weeks. Top UK doctor: Ebola screening should be improved Ebola epidemic Photo: AP Medical staff in protective clothing transport a healthcare worker diagnosed with the Ebola virus disease in a quarantine tent prior to her being transferred to the Royal Free Hospital in north London at Glasgow airport, Scotland, Tuesday, Dec. 30, 2014. A British health care worker who contracted the Ebola virus in West Africa has been transferred from Scotland to an isolation unit in London for specialist treatment. Show more Ebola epidemic Photo: APMedical staff in protective clothing transport a healthcare worker diagnosed with the Ebola virus disease in a quarantine tent prior to her being transferred to the Royal Free Hospital in north London at Glasgow airport, Scotland, Tuesday, Dec. 30, 2014. A British health care worker who contracted the Ebola virus in West Africa has been transferred from Scotland to an isolation unit in London for specialist treatment. Show more LONDON (AP) — Britain's Ebola screening procedures should be improved, the country's chief medical officer said Wednesday, after a nurse was cleared to fly hours before she was diagnosed with the disease. Nurse Pauline Cafferkey flew from London to Glasgow on Sunday after returning from Sierra Leone. Her temperature was taken seven times at Heathrow Airport — once on arrival and six times after she told staff she thought she might have a fever. Her temperature was found to be within the range defined as acceptable, and she was allowed to fly to Scotland. Cafferkey developed a fever Monday and is being treated in an isolation unit at a London hospital. A doctor who flew back from Sierra Leone with Cafferkey, Martin Deahl, has criticized the Heathrow screening, saying there were too few staff and the medical workers were not segregated from other passengers. Chief Medical Officer Sally Davies said that "the process does seem to have not been as good as we all want to see." But she said Cafferkey had not been showing symptoms and posed little risk to fellow passengers. She said screening procedures for people returning from West Africa are being reviewed. Cafferkey is the first person diagnosed with Ebola on British soil. Doctors at the Royal Free Hospital in north London said she was being treated with an experimental antiviral drug and with plasma from a recovered patient containing Ebola-fighting antibodies. Infectious diseases specialist Dr. Michael Jacobs said Cafferkey was sitting up and able to eat, read and talk to her family. He said the patient was in "a positive frame of mind," although "I'm sure this isn't how she intended to spend New Year's Eve." Since an Ebola outbreak began in December 2013 in the West African country of Guinea, there have been about 20,200 cases and about 7,900 deaths, mostly in Liberia, Guinea and Sierra Leone, according to figures released Wednesday by the World Health Organization. Health December 31, 2014 Top UK doctor: Ebola screening should be improved LONDON (AP) — Britain's chief medical officer acknowledged Wednesday that Ebola screening procedures should be improved, after a nurse was cleared to fly hours before she was diagnosed with the disease. Nurse Pauline Cafferkey flew from London to Glasgow on Sunday after returning from Sierra Leone. Her temperature was taken seven times at Heathrow Airport — once on arrival and six times after she told staff she thought she might have a fever. Her temperature was found to be within the range defined as acceptable, and she was allowed to fly to Scotland. Cafferkey developed a fever Monday and is being treated in an isolation unit at a London hospital. A doctor who flew back from Sierra Leone with Cafferkey, Martin Deahl, has criticized the Heathrow screening, saying there were too few staff and the medical workers were not segregated from other passengers. Chief Medical Officer Sally Davies said that "the process does seem to have not been as good as we all want to see." But she said Cafferkey had not been showing symptoms and posed little risk to fellow passengers. She said screening procedures for people returning from West Africa are being reviewed. Cafferkey is the first person diagnosed with Ebola on British soil. Since an Ebola outbreak began in December 2013 in the West African country of Guinea, there have been more than 20,000 cases and more than 7,800 deaths, mostly in Liberia, Guinea and Sierra Leone. Taiwan reports suspected Ebola infection English.news.cn 2014-12-06 13:26:01 More TAIPEI, Dec. 6 (Xinhua) -- Taiwan's disease control authorities said on Saturday that a 19-year-old man is suspected of being infected with the Ebola virus. The man has developed symptoms of vomiting and diarrhea since he returned from Nigeria, where he had contact with animals, the authorities said. He is now isolated in a hospital in Kaohsiung City, southern Taiwan. Samples have been sent to Taipei for examination, and authorities will announce the result this afternoon. The authorities called on people to stay calm and have a check-up after returning from West Africa. Ebola death toll in West Africa becomeming 'unpalatable,' expert says Health December 08, 2014 LONDON (AP) — As health officials struggle to contain the world's biggest-ever Ebola outbreak, their efforts are being complicated by another problem: bad data. Having accurate numbers about an outbreak is essential not only to provide a realistic picture of the epidemic, but to determine effective control strategies. Dr. Bruce Aylward, who is leading the World Health Organization's Ebola response, said it's crucial to track every single Ebola patient in West Africa to stop the outbreak and that serious gaps remain in their data. "As we move into the stage of hunting down the virus instead of just slowing the exponential growth, having good data is going to be at the heart of this," Aylward said. "We are not there yet and this is something we definitely need to fix." "Decisions about prevention and treatment should be data-driven, but we really don't have the data," agreed Irwin Redlener, director of the National Center for Disaster Preparedness at Columbia University. A week ago, the World Health Organization insisted at a media briefing it had mostly met targets to isolate 70 percent of Ebola patients and bury 70 percent of victims safely in Guinea, Liberia and Sierra Leone. But two days later, WHO backtracked and said that data inconsistencies meant they really didn't know how many patients were being isolated. Then the U.N. health agency also conceded that many of the safe burials were of people not actually killed by Ebola. Aylward said not knowing exactly how many Ebola patients there are in hotspots like western Sierra Leone means health officials might miss potential contacts who could unknowingly cause a surge of cases. Compared to other epidemics like malaria, which is more seasonal and can fade away without huge control efforts, ending the Ebola outbreak will require extraordinary attention to detail. "This outbreak started with one case and it will end with one case," Aylward said. "If we can't get 100 percent of the contacts of cases, we will not be on track to shut it down. Unfortunately at the moment, the data right now is not enough for us to get to zero." In West Africa, where health systems were already broken before Ebola struck, collecting data amid a raging outbreak has been challenging. "Suddenly you have all these different sources of data that have to be compiled" from different aid agencies, said Ray Ransom, a data expert at the U.S. Centers for Disease Control and Prevention. "The ability to actually collect information is a different challenge than responding to the outbreak, and the energy has been focused on the response." He said local officials are good at tracking known or suspected Ebola cases and their contacts but not as reliable relaying that information to national authorities. The software built to track Ebola outbreaks was initially designed by the CDC to have one person entering data into a computer. That "was perfectly fine since the dawn of time up until" the outbreak exploded this summer, said Armand Sprecher, a public health specialist with Doctors Without Borders. The CDC has redesigned the software so now multiple people can enter data, although that created new problems like possible duplication, Sprecher said. When the epidemic starts to taper off, health officials should have more time to find every Ebola case and their contacts. But they may find they have to re-establish trust with the community to do that. "If people were calling in cases for months and no one was coming ... and then suddenly that's no longer a bottleneck, do people suddenly realize that and say, aha, if I call in today, it'll work this time?" asked Sprecher. "If you've lost the community, you don't get anywhere." LONDON (AP) — As the biggest-ever outbreak of Ebola continues to ravage West Africa, here are a few key numbers to get a handle on the epidemic: 13,268 and 4,960: According to an update Friday from the World Health Organization, there have been 13,268 Ebola cases and 4,960 deaths since the first child died of the virus in December — but those figures include all probable, suspected and confirmed cases and are subject to change as more information becomes available. The numbers fluctuate as more data becomes available, and as probable and suspected cases are either discarded or confirmed. Experts warn the actual number of cases and deaths are likely far higher than what's been reported, because people may be reluctant to seek care and officials are too overwhelmed with control efforts to record every single case. The vast majority of patients are in Guinea, Sierra Leone and Liberia. Cases and deaths are typically only recorded days after people become symptomatic or die, which complicates a real-time understanding of Ebola. "We are definitely getting a delayed picture of the outbreak," said Sebastian Funk, a lecturer in infectious diseases at the London School of Hygiene and Tropical Medicine. "It's difficult to tell if we are reaching a turning point or if there will be a doomsday scenario. I could see it going either way at the moment." 4,707: According to WHO, 4,707 beds are needed across West Africa in Ebola treatment clinics; at the moment, just 22 percent of the necessary number are operational. The agency estimates a further 2,685 beds are needed for basic Ebola clinics where minimal treatment is provided and people are mostly isolated while waiting for test results. At the moment, just 4 percent of beds in these community clinics are available. Given the uncertainty around case numbers, Funk says things like bed occupancy are a good sign of how the outbreak is evolving. "We really need to see numbers go down for several weeks to be confident it's a real trend," he said. 549: WHO reports that 549 health workers have been infected with Ebola, of whom 311 have died. Since Ebola is spread via contact with the bodily fluids of a patient, health workers are at high risk of catching the disease. The U.S. Centers for Disease Control and Prevention recommends that no skin be showing in a health worker treating Ebola patients. Eight: There are now eight countries that have reported Ebola detected on their soil: Guinea, Liberia, Sierra Leone, Mali, Nigeria, Senegal, Spain and the U.S. Other countries like Britain, France and Germany have taken in people sickened by the deadly virus in West Africa but they have not reported any spread of the virus there. Four: There have been four cases of Ebola diagnosed in the U.S. and a single death — Thomas Eric Duncan, the Liberian man who was the first person diagnosed with Ebola in the country, who later died at a Dallas hospital. Two cases were nurses who cared for Duncan. The fourth is a New York doctor who became sick a week after returning from West Africa. Two: It took two months for Britain to build and open its first Ebola treatment center in Sierra Leone this week, an 80-bed facility with a dozen other beds reserved for infected health workers. The Kerry Town clinic, near the capital, Freetown, is the first of six centers to be built by the U.K. in Sierra Leone. It includes a triage center, ambulance pads, laboratory, pharmacies and decontamination units. In about the same time that it took to build the Ebola clinic, Sierra Leone has reported more than 3,500 cases of Ebola. One: There is one remaining American hospitalized with Ebola, Dr. Craig Spencer in New York, a physician who worked for Doctors Without Borders in Guinea. He continues to show improvement, remains in isolation and is in stable condition. The Department of Homeland Security (DHS) has announced all travelers from the West African countries stricken with Ebola must travel to the U.S. through one of only five airports. Travelers from Liberia, Sierra Leone and Guinea are being forced to travel through the five airports previously announced as Ebola screening centers for international travelers, officials said in a statement. Those five airports are New York-JFK, Newark Liberty, Washington, D.C. Dulles, Atlanta Hartsfield-Jackson and Chicago O'Hare. All passengers taking flights from West Africa to these five airports will be subject to "secondary screening and added protocols, including having their temperature taken, before they can be admitted into the United States," officials said. "We are working closely with the airlines to implement these restrictions with minimal travel disruption," said DHS secretary Jeh Johnson. "If not already handled by the airlines, the few impacted travelers should contact the airlines for rebooking, as needed." There presently are no direct flights from those countries into the U.S. It was also further announced that any passengers who have traveled into the country from West Africa during the preceding 21 days will also be screened for the deadly virus. The restrictions come one month after Liberian national Thomas Duncan arrived in Dallas on September 20. He died October 8 from Ebola and two nurses have subsequently become infected. "The Department of Homeland Security's policy to funnel all passengers arriving from Ebola hotspots to one of these five equipped airports is a good and effective step towards tightening the net and further protecting our citizens," said Senator Charles Schumer (D-NY). This may be the first of many steps aimed at stemming the flow of infected people into the U.S. "We are continually evaluating whether additional restrictions or added screening and precautionary measures are necessary to protect the American people and will act accordingly," said Johnson. Growing concerns about a possible Ebola outbreak in Mali have at least one expert concerned many more people will die from the deadly disease than previously thought. More than 5,100 people have died in West Africa from this year's outbreak across Guinea, Liberia and Sierra Leone. Four have died from Ebola in recent weeks in Mali and authorities are scrambling to track down another 250 individuals for monitoring. A further 14,413 are known to be infected, and the death toll among them is reaching 70 percent, according to the World Health Organization (WHO). This is the largest Ebola outbreak in history. Those deaths are believed have been people infected by a Guinean imam who died in Mali of the disease, according to the WHO. But another outbreak in the country is raising fears that infections may be more widespread. Many experts, including Jennifer Nuzzo, a leading infectious disease expert with the University of Pittsburgh Medical Center, sees the spread of Ebola to Mali as a potential "game changer" but is hopeful the outbreak can be quickly contained. "I'd like to think it's not community-wide," Nuzzo told AOL News, "but it's not surprising to find more cases. "Hopefully they can put a ring around them and extinguish the disease," she added. Nuzzo contends there is reason to worry, but expressed hopes that efforts to contain the disease in Mali are as effective as in Nigeria. A recent infection in Lagos, a teeming city of about six million people, was isolated and cured almost as quickly as a New York doctor who became in infected after returning from treating Ebola-stricken patients in Guinea. "Everybody was really worried about Nigeria," said Nuzzo. Experts have since instead been focusing their attention on Sierra Leone, where infections appeared to slow a bit before picking up again. "Sierra Leone is doing far, far worse than it had in a long time," said Nuzzo. The rising number of infections, combined with those already infected in Guinea and Liberia, mean it is going to be a long road to recovery, according to Nuzzo, who believes the death count could easily rise higher than previous prediction. "I think its not going to be palatable," she said. Previous Ebola outbreaks have been confined mostly to villages, but this one has hopped the borders of six countries, and Mali shares a 500-mile border with Guinea. "The fact we're now seeing cases Mali, and Sierra Leone seems to be heating up, shows that we are in this for the long haul," said Nuzzo. The desperation of people looking for a cure has led them down many a dark path, including the use of arsenic and snake venom, according to the Daily Mail. Doctors Ortrud Lindemann, from Germany, and Richard Hiltner, from California, set off for Liberia recently to prove the two toxins would prove effective as homeopathic Ebola cures, according to the British newspaper. Nuzzo slammed the idea, saying that there is virtually no way either could be effective treatments for the lethal disease. "I don't know of any reason why those two things would work on a virus like Ebola," said Nuzzo. "It doesn't seem really feasible." Both arsenic and snake venom are toxic to humans, even at small amounts of exposure, and U.S. authorities have worked for decades remove arsenic, which occurs naturally, from the nation's water supply. "You're talking about arsenic ... a known poison, its pretty remarkable," said Nuzzo. "If the Ebola doesn't kill you, the arsenic will." The only way to bring the deadly disease under control, according to Nuzzo, is to bring an Ebola vaccine to reality. Clinical trials of a potential vaccine and other treatments still ongoing, it is not known how soon they can be approved by health officials. The best way to at least slow the infection rate until then, says Nuzzo, is to not demonize with onerous mandatory quarantines the doctors returning from Africa after stints volunteering to help fight the disease. "I worry that, what we are doing, it sounds like we're going to make it harder to stop the outbreak." GENEVA: The World Health Organisation said on Wednesday (Nov 12) that 5,160 people have so far died of Ebola across eight countries, from a total 14,098 cases of infection. The numbers supersede figures the UN health agency gave last Friday, when it reported 4,960 deaths and 13,268 cases. WHO has acknowledged though that the number of deaths is likely far higher, given that the fatality rate in the current outbreak is known to be around 70 per cent. The fresh toll, which runs through Nov 9, comes as the outbreak appeared to be spreading in Mali, with four Ebola cases, all of whom died, confirmed or suspected in that country. The deadliest Ebola outbreak ever meanwhile continues to affect Guinea, Liberia and Sierra Leone the most. In its latest toll, the WHO said 2,836 deaths were recorded in Liberia, out of a total of 6,822 cases. In Sierra Leone, 1,169 people had died from the virus out of 5,368 cases. In Guinea, there were 1,142 deaths from 1,878 cases. Data from Nigeria and Senegal remained unchanged, and both countries have been declared Ebola free. Nigeria had eight deaths and 20 cases, while Senegal had one case and no deaths. In Mali, WHO reported three additional Ebola deaths, but said they were not linked to the only other case and death recorded in the country - that of a two-year-old girl from Guinea. There has been one case of infection in Spain, where an infected nurse has recovered. In the United States, four Ebola cases have been recorded and one person - a Liberian - had died from the virus. Ebola, one of the deadliest viruses known to man, is spread only through direct contact with the bodily fluids of an infected person showing symptoms such as fever or vomiting. People caring for the sick or handling the bodies of people infected Ebola are therefore especially exposed. WHO said on Wednesday that a total of 564 healthcare workers were known to have contracted the virus, and 320 of them had died. 2014年11月06日 预防措施 预防措施: 卫生防护中心人员在演习期间,把可能沾上病人体液的床铺收集弃置。 上一则下一则 卫生署卫生防护中心今日在尖沙咀旅馆举行代号「托帕」的演习,模拟有旅客确诊感染伊波拉,测试当局的应变计划,找出需要改善之处。 演习期间,卫生防护中心派员到旅馆进行流行病学调查,确认可能的感染源头、相关接触者、被病人体液污染的地方和物件,食环署人员随即在房间和升降机大堂消毒。 是次演习旨在实地测试卫生署和食物环境卫生署人员在调查和消毒工作的协调,也让大厦管理处了解一旦有病人确诊感染时需要采取的措施。 2014年11月6日 有关埃博拉(伊波拉)病毒病的资讯 政府「埃博拉(伊波拉)病毒病准备及应变计划」下的戒备应变级别现正启动 埃博拉(伊波拉)病毒病 埃博拉(伊波拉)病毒病是由感染埃博拉(伊波拉)病毒所致。潜伏期为2至21天。病人可能出现突发性发烧、极度虚弱、肌肉疼痛、头痛和咽喉痛。随后会出现呕吐、腹泻、皮疹、肾脏和肝脏功能受损,在某些情况下更会出现内出血和外出血。人类感染的死亡率可高达90%。 埃博拉(伊波拉)病毒是通过密切接触受感染动物而传到人类。随后通过人际间传播,传播途径包括直接接触(通过破损皮肤或黏膜)感染者的血液、分泌物、器官或其他体液,以及间接接触受到这类体液污染的环境。 现时没有认可预防埃博拉(伊波拉)病毒病的疫苗。要预防感染疾病,游客必须要注意以下数点: 尽量避免到受影响地区旅游 注重个人和环境卫生;在接触眼、鼻及口前切记先以梘液或酒精搓手液清洁双手 避免密切接触发烧人士或病人,并避免接触患者的血液、体液和可能接触过患者血液或体液的物品 避免接触动物 食物须彻底煮熟才可进食;及 市民如从受影响地区返港,应留意返港后21日内的健康情况。如在这段时间出现埃博拉(伊波拉)病毒病的病征,应致电999并告知人员有关情况,以安排到急症室求诊 // 俄国新闻 / 卫生保健 |
|
俄消费者权益保护局:俄提出加强对抗埃博拉病毒方案
|
|
17:52
| 2014-10-21
|




核心提示:今年4月暴发的埃博拉病毒疫情,目前已经在几内亚、利比里亚与塞拉利昂西非三国造成数千人死亡,且未有被控制住的迹象。

9月22日,中国人民解放军援塞医疗队队员正在向塞拉利昂人员讲解传染病防治知识。 新华社

9月28日,中国实验室检测队队员正在中塞友好医院内与塞方交接埃博拉病毒样品。新华社
危难之际显真情。中国向遭受疫情的非洲国家伸出了援助之手:第一时间向非洲疫情国家提供防控救治物资,8月再次紧急提供价值3000万元的人道主义物资,9月再次提供2亿人民币紧急援助。另外,中国向塞拉利昂提供了移动生物实验室。
难能可贵的是,中国分别向西非三国派遣了医疗专家队伍,冒着被感染风险与当地民众并肩作战,他们是离致命病毒埃博拉最近的人、也是最勇敢的人。美国医护人员日前被感染上埃博拉病毒的消息,更是增加了他们的风险。
本文是《国际先驱导报》驻塞拉利昂记者发回的报道,近距离记录了这批离致命病毒最近的中国医生工作与生活的细节。
《国际先驱导报》记者 林晓蔚 发自弗里敦(塞拉利昂)
塞拉利昂地处西非,盛产钻石,一度因为“血钻”而世界闻名。令该国生灵涂炭的十余年内战,便是因政府与反对派争夺钻石产区而起。近年来,逐步摆脱内战阴影的塞拉利昂正在享受经济腾飞,连年GDP增长率在10%以上,成为非洲经济的耀眼明星。
但2014年的塞拉利昂迎头撞上了神秘的埃博拉病毒,这种几十年来忽隐忽现,至今“无解”,死亡率极高的致命病毒,从几内亚蔓延到了利比里亚和塞拉利昂西非三国,数千人因此去世,并进一步引发了全球性恐慌,世人谈之色变。
在这样的节骨眼上,中国决定成为伸出援手的大国一员。自8月中旬始,中国疾控中心陆续派出专家组进行前期调研、现场走访,积累一手材料,这一切都是在为9月中下旬的一次重量级行动做准备——派驻移动实验室和前线医疗队。
如今,实验室和医疗队在塞国首都弗里敦市郊的中塞友好医院已工作一月。他们情况如何?实验室平时工作情形是怎样的?医疗队队员们如何在接诊埃博拉患者的过程中与死神赛跑?

绕行三个半小时进首都
9月17日凌晨2时许,一支59人的中国专家队伍搭乘专机抵达塞拉利昂首都弗里敦的隆吉国际机场。平日里,机场和市区间的交通是40分钟海上快艇,当夜,为安全起见,全体队员经陆路绕行塞国西部省半岛返回首都,耗费3个半小时。
在接机的中国援塞医疗队队长王耀平手机里,还保存着当时的照片:清晨,天已大亮,经历长途飞行的队员们,或靠在椅背上闭目养神,或好奇地看着窗外的景色,或小声讨论着下一步的计划与部署。雨季还未过去,中国人已经来了。
59人当中,29人来自中国疾控中心(CDC),负责移动实验室的日常运作;30人来自解放军302医院,负责在中塞友好医院直接接诊埃博拉疑似病例。“首日即是首战开始。”当天上午抵达酒店后,两支队伍便各自投入实地考察,并无任何休息。
18日凌晨4时许,弗里敦下起了倾盆暴雨,随货机运抵的物资不少都泡在了水里,专家们亲自上阵,和使馆协调派来的搬运工一道冒雨将物资搬进临时库房。经过8个小时连续工作,库房里放满了9辆大卡车运来的物资。
9月19日至21日,弗里敦几乎成了一座空城。这是因为塞拉利昂政府决定所有人在家闭户3日,挨家挨户搜查有无埃博拉病例的“漏网之鱼”。在这次为期3天的大搜查中,该国又找出了百余例疑似患者,美国、加拿大、南非等国驻塞病毒检测实验室开始“加班加点”。
在中国驻塞拉利昂使馆的协调下,几家至今仍留守在该国的建筑类中资企业纷纷派出了自己的工人前来中塞友好医院,参与医院的布局改造。
自抵达后,不到10天时间,解放军援塞医疗队队长李进便向记者透露,中塞友好医院已经符合烈性传染病防治流程,病例留观中心即将开始运作。

租俄运输机运送实验室
与此同时,塞拉利昂时间9月25日晚,一架从俄罗斯租用的“安-124”大型运输机降落在隆吉国际机场,中国移动实验室终于运抵塞拉利昂。这座具有独立知识产权,价值逾千万元人民币的生物安全三级实验室,第一次走出国门,即是远赴西非对抗埃博拉病毒。
中国疾控中心此次派来的检测队队长钱军,同时也是移动实验室主任。这名经验丰富的卫生防疫专家向记者详细介绍了移动实验室的方方面面。
实验室由3台独立方舱组成:主舱、辅舱和中控指挥舱,内部设备包括手套箱隔离器、生物安全柜、自控充气式气囊门、自洁净型传递窗、高压污物灭菌器、高效充气过滤器以及高温污水煮沸罐等。
实验室按照“四流”(人流、物流、气流、水流)控制理念,遵循“三区两缓两传递”标准设计,实现了对“三废”(废水、废气、废物)的无害化处理,它同时装有车载水、电保障系统,可车载、空运、海运以及铁路运输,具备“日行千里”的机动能力。检测队技术保障组组长王承宇说,每天实验室启动前,他们都要检查发电站和水循环系统,逐项排查电力、水路、气路、实验室压力、温度、送排风高效过滤器等是否正常,通讯、视频监控系统是否良好。
“实验开始后,还要全过程对实验进行监督指导,对存在的安全隐患进行及时纠正;实验结束后,要对废弃物进行高压灭菌与焚烧销毁,定期进行实验仓消毒处理。”王承宇透露。
据王承宇介绍,实验室的运转需要充足的水、电、油供应,这在几乎每天停电数次时不时出现油荒的塞拉利昂是个挑战。“这里不像国内,各项保障条件都难以达到国内的标准,甚至一颗螺丝都无法买到。”王承宇说,实验室一旦出现故障,就有可能酿成重大的生物安全事故。因此,技术保障组的5名组员,每天都像“看护自己的眼睛”一样守护着实验室,从供水、供电、供油、通信、监控等基本工作抓起,时刻处理哪怕是再小的机械问题。
防护服穿脱有36道流程
10月1日,中塞友好医院埃博拉留观中心正式启用。当日,解放军援塞医疗队接诊了两批共7名留观患者。当天一早,6人医护小组就全副武装做好准备,第一辆救护车运来首批5名患者后,防控组即刻对车辆进行彻底消毒。
首批患者3名女性、2名男性,年龄最大24岁,最小只有8岁,从救护车上下来后,患者因四肢乏力、头痛、呕吐等现象严重,全部躺倒在门诊大厅前的台阶上。护士孙娟逐一发放口罩并引导到门诊,治疗组组长秦恩强进行初步诊断。据解放军援塞医疗队队长李进介绍,护士为每名患者在腋下粘贴新型无线体温计后,可以通过体温远程连续监测及预警系统,每天连续自动采集发送体温测量数据,以有效减少交叉感染和病毒传播。
经记者细数,中国一线医护人员防护用品共有11件,其中包括防护服、防护口罩、护目镜、隔离衣、手套、防水雨靴等,穿,共有13道流程;脱,则多达23道。每脱一件防护用品,都要对手部进行一次消毒,并严格规定从上到下穿戴。口罩先戴后摘,穿脱不颠倒,行走不反向,脱防护服忌抖动等10条原则要求。
据介绍,留观中心内先期展开的床位目前有40张,分设疑似和确诊两个病区。安装的远程监控设备,不但实现工作人员缓冲区、接诊台、药房以及确诊患者病房等重点部位全覆盖,而且还可将污染区的病历资料传输到清洁区,确保病历资料的清洁和完整。
被转运来的留观病人,由于未经检测,暂时无法判断,一律安排住单间隔离病房。“这样做的目的就是想控制传染源、切断传播途径,有效预防交叉污染。”医疗队医疗保障组组长郭桐生对记者说。
留下“永不撤退”的防疫队伍
9月28日下午14时26分,中塞友好医院传出了实验室检测队队员鲁会军、孙洋的一线报告,中国卫生防疫专家成功检出第一批埃博拉病毒样品。“这是我国援塞实验检测队的首例,也是中国抗击埃博拉疫情的首例。”钱军说。
10月2日,实验室检测队接检埃博拉病毒样品已破百例,其中共检测出阳性样本62例。截至当日,在接检的121份样本中,约半数来自于该国首都弗里敦及周边的西部省,这也是该国近期疫情急剧攀升、形势最为严重的地区。这些数据,对于塞拉利昂政府确诊住院患者、做好尸体处理及隔离工作,起着十分重要的指导作用。
“队员们平均每天工作达12小时以上。”据钱军透露,塞拉利昂方面反馈称,中国实验室检测结果无一差错。
钱军说,这是中国公共卫生防疫专家第一次一线接触并实毒操作如此烈性的传染病毒,也是中国卫生专家人员、技术、装备第一次跨国界独立开展工作,可以说是“摸着石头过河”。
截止10月8日,中国实验室检测队接检埃博拉病毒样本累计290例,已占检测队抵塞开展工作以来该国检测样本总数的23%,其中阳性样本157例,大部分来自该国包括首都弗里敦在内的西部省,接近该省检出阳性样本的半数。
“我们的团队是过硬的,移动实验室是‘争气’的,检测技术是经得起考验的。”尽管连日作战让声音中听起来有几分疲惫,说到这些时钱军仍然提高了音量。
他透露,国内已经有了下一步的初步方案,计划在中塞友好医院附近为塞拉利昂建造一座固定生物安全防护三级实验室,所需设备、器材等都在筹备之中,预计数月内将建成并投入使用。
“中国政府和专家将积极为塞国培训相关防疫专家和人才,也可利用移动实验室进行实地培训,等固定实验室投入使用后,中国专家也可能来塞拉利昂进行指导帮助。”钱军说,要为塞拉利昂留下一支“永不撤离”的卫生防疫队伍。
俄新网RUSNEWS.CN莫斯科10月21日电 派往几内亚首都的俄罗斯消费者权益保护和公益监督局专业防疫队负责人瓦连京·萨夫罗诺夫向俄新社表示,加强控制西非埃博拉病毒扩散的工作需要调整,俄罗斯有一系列相关建议。
他表示:“加强控制病毒扩散的工作需要调整,俄罗斯有一系列建议。”他指出,俄罗斯消费者权益保护和公益监督局的具体建议将在晚些时候公布。
他说,现在很难说出消除瘟疫的日期,但存在将影响瘟疫持续时间的因素。
此前萨夫罗诺夫会见了几内亚总统阿尔法·孔戴。总统对俄罗斯专家帮助对抗埃博拉表示感谢。总统还希望俄罗斯将继续帮助对抗病毒。
俄罗斯消费者权益保护和公益监督局专业防疫队从8月22日开始逗留几内亚首都科纳克里。防疫队包括病毒学家、流行病学家和微生物学家,他们负责诊断病毒。他们的任务包括人道援助几内亚居民、诊断和保护该国境内的俄罗斯公民。
据世界卫生组织资料显示,已经有4500多人死于西非爆发的埃博拉病毒。
防控埃博拉病毒,我们能做什么?
2014年10月21日13:58 来源:人民网-健康卫生频道  手机看新闻
手机看新闻
人民网北京10月21日电 埃博拉出血热是一种严重且往往致命的疾病,病死率最高可达90%。目前疫情已扩散到非洲以外,在美国、德国、西班牙等国均发现埃博拉病毒感染者。预防埃博拉,个人可以做什么?中国疾病预防控制中心介绍,采取推荐的保护措施可以控制或阻断疾病的传播,一旦出现相关症状应立即就医。
图片源自网络
什么情况下容易感染?
接触传播是本病最主要的传播途径。可以通过接触病人和被感染动物的血液、体液、分泌物、排泄物及其污染物感染。
病例感染场所主要为医疗机构和家庭,在一般商务活动、旅行、社会交往和普通工作场所感染风险低。病人感染后血液中可维持很高的病毒含量。医护人员、病人家属或其他密切接触者在治疗、护理病人或处理病人尸体过程中,如果没有严格的防护措施,容易受到感染。
人们应当何时就医?
感染埃博拉病毒的典型症状和体征包括突起发热、极度乏力、肌肉疼痛、头痛和咽喉痛。随后会出现呕吐、腹泻、皮疹、肾脏和肝脏功能受损,某些病例会同时有内出血和外出血。
人们若去过已知存在埃博拉病毒的地区,或与已知或疑似携带埃博拉病毒的人员接触过,当开始出现症状时,应立即就医。
当怀疑病人患有该病时,应当立即向最近的卫生机构报告。及时就医对提高患者的生存率至关重要。同时应加强感染控制,以控制疾病传播。
如何看待某些食物可预防或治疗感染的传言?
世界卫生组织(以下简称WHO)强烈建议,人们应从公共卫生机构获取埃博拉出血热方面的健康建议。
目前没有针对埃博拉出血热的特异性药物,最佳的治疗方法就是在严格的感染控制程序下,由医院的医务人员对病人进行强化性的支持治疗。按照推荐的保护性措施去做,就可控制感染的发生。
相关报道:
目前,在美国埃博拉病毒已使多人感染:最早的两起传播病例是两位护士,她们在护理过美国第一位埃博拉确诊病人托马斯·邓肯(Thomas Duncan)之后出现了感染症状。在达拉斯德州健康长老会医院(Texas Health Presbyterian Hospital)收治邓肯的10天期间,有70多名医护人员与该患者有过接触,其中两名护士妮娜·范(Nina Pham)和安布尔·乔·文森(Amber Joy Vinson)染上了埃博拉病毒。然而,周三该医院的一些员工在接受匿名采访时表示
![]()



